
Hypoxia
The ‘cabin altitude’ in commercial aircraft should not exceed 8000 feet in normal operations, but in practice is typically between 5,000 and 7,500 feet. This results in a concomitant decrease in the partial pressure of alveolar oxygen (PAO2) - at the upper limit of cabin altitude of 8,000 feet, the cabin pressure is approximately 565 mm Hg and P AO2 is approximately 75mm Hg. However, due to the shape of the oxy-haemoglobin dissociation curve (Figure 1), this only results in a fall of arterial oxygen saturation to around 90% and is well tolerated in healthy travellers. Passengers with medical conditions associated with hypoxia or reduced oxygen-carrying capacity in the blood, such as respiratory and cardiac conditions or severe anaemia, may not tolerate the reduction in barometric pressure without additional support.
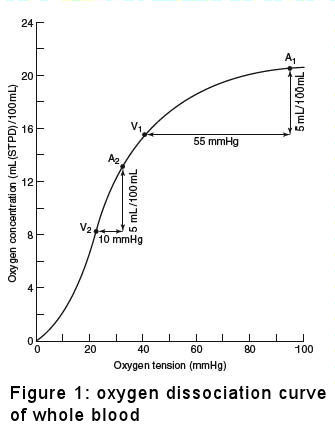
Figure 1
Extract from Ernsting’s Aviation Medicine, Edited by Rainford D J, Gradwell D P. Fourth Edition. Chapter Title, Authors, © 2006 Edward Arnold (Publishers) Ltd.
Reproduced by permission of the publisher.
Barometric pressure
The decrease in ambient pressure in the cabin as the aircraft climbs to its cruising altitude will cause any gas to increase in volume by approximately 30%. As the aircraft descends to land, the increasing cabin pressure will lead to a corresponding reduction in volume. Gas within body cavities may cause problems if it is trapped and unable to expand freely or if there is obstruction to the free flow of air preventing equalisation of air pressure. The effects of this are most commonly seen in passengers suffering from upper respiratory tract infections, who may suffer ear or sinus pain and bleeding (otic / sinus barotraumas). Similar and potentially more serious issues may occur following surgery, if gas is introduced to the abdominal cavity or the eye, or in people with lung bullae or an non diagnosed pneumothorax.
There is also a potential for interference with the function of medical devices, such as insulin pumps, as a result of formation/expansion of air bubbles.
Humidity and hydration
The ambient air at typical aircraft cruising altitudes has very low levels of water vapour and as a result the humidity levels in the cabin are typically in the range 10 to 20% compared to that in buildings, which is in the order of 40 to 50%. However, contrary to a widely held belief, the low humidity in the aircraft cabin does not result in dehydration. Research has shown that the additional insensible fluid loss amounts to approximately 150ml over an 8 hour flight, with no evidence of any change in plasma osmolality. This increased fluid loss would readily be compensated by the normal homeostatic mechanisms. The low humidity may result in drying of the mucous membranes of the lips and tongue, leading to a sensation of thirst, and can also cause problems for contact lens wearers due to corneal drying.
Jet lag
Jet lag or circadian dysrhythmia is a consequence of trans meridian travel and, as well as being an annoyance for travellers may be of medical significance for passengers who require regular medication. Consideration should be given to the timing of medication, e.g. in patients with diabetes who are treated with insulin or HIV positive patients on ART.
Provide page feedback
Please enter your comments below, or use our usual service contacts if a specific matter requires an answer.
Fields marked with an asterisk (*) are required.